Patient Information from ISHA – The Hip Preservation Society
Pubic Symphysis Pain – Pubalgia
Pubic Symphysis Pain - Pubalgia
Definition
Pubalgia is a condition characterised by chronic pain in the pubic or groin area. It is usually triggered by activities requiring significant physical effort and is more common in sports that require sudden changes in direction or repetitive kicks, such as soccer or hockey. This condition is prevalent in athletes, varying from 3 to 11% in Olympic athletes and from 10 to 18% in professional soccer players.
Causes
There are three main causes of pubalgia:
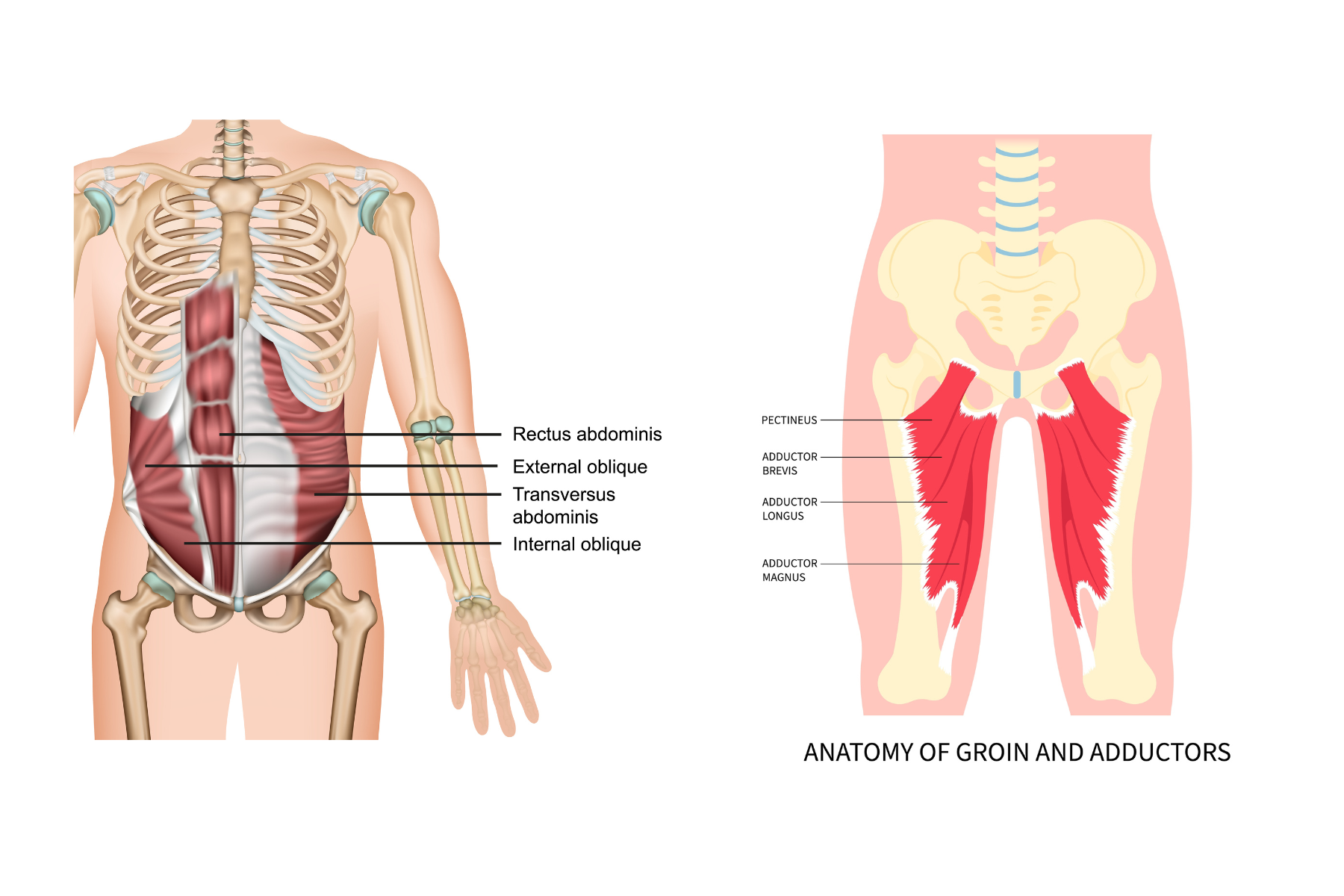
Muscle imbalances or overload between either the hip adductor and abdominal muscles, or between the hip adductor and abductor muscle groups.
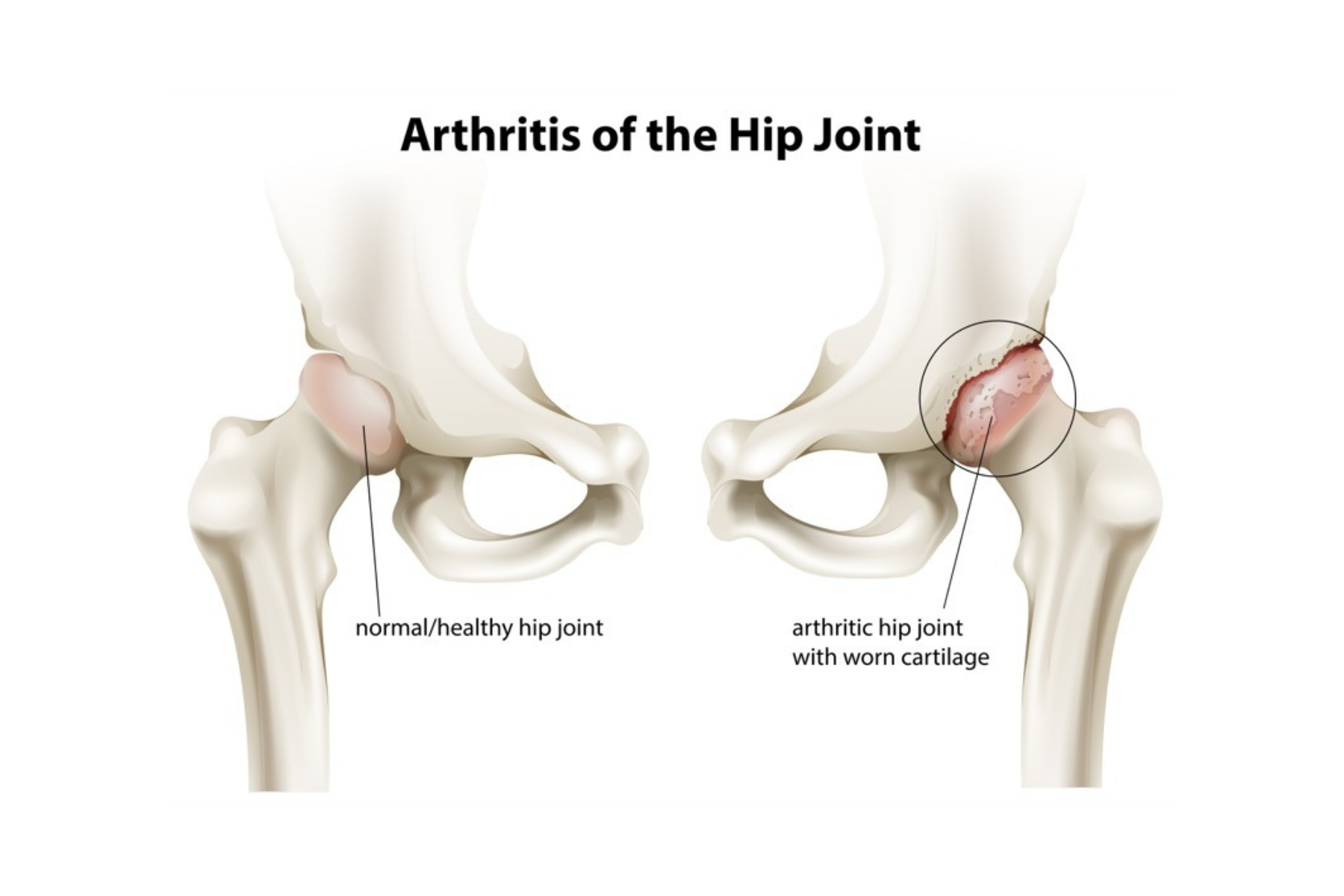
Mechanical stress on the pubic symphysis due to femoroacetabular impingement (FAI) or reduced range of motion at the hip joint, as seen with osteoarthritis or where rotational abnormalities of the femur exist.

Inguinal (groin)-related pain due to posterior abdominal wall weakness (also called “sports hernia”), which can lead to bulging of the abdominal muscle wall, compressing nearby nerves. In some cases, true direct or indirect hernias can be the cause of pain.
Signs and Symptoms
- Pain, which can be on one side or both, and located around the groin, lower abdomen, over the area of the pubic symphysis, perineal region, inguinal region or scrotum
- Extreme tenderness over the region of the pubic symphysis
- Pain during abdominal or adductor muscle contractions, aggravated by kicking, running, or from eccentric loading to the rectus abdominis
- Reduced range of movement at one or both hips
- Pain ranging from mild discomfort to debilitating, sharp shooting pains either at the front or back of the pelvis as well as aching in areas such as the abdomen, back, groin, perineum, thigh and leg
- Pain aggravated by walking, bending forwards, climbing up or down stairs, getting in and out of chairs and cars, and turning in bed
Diagnosis
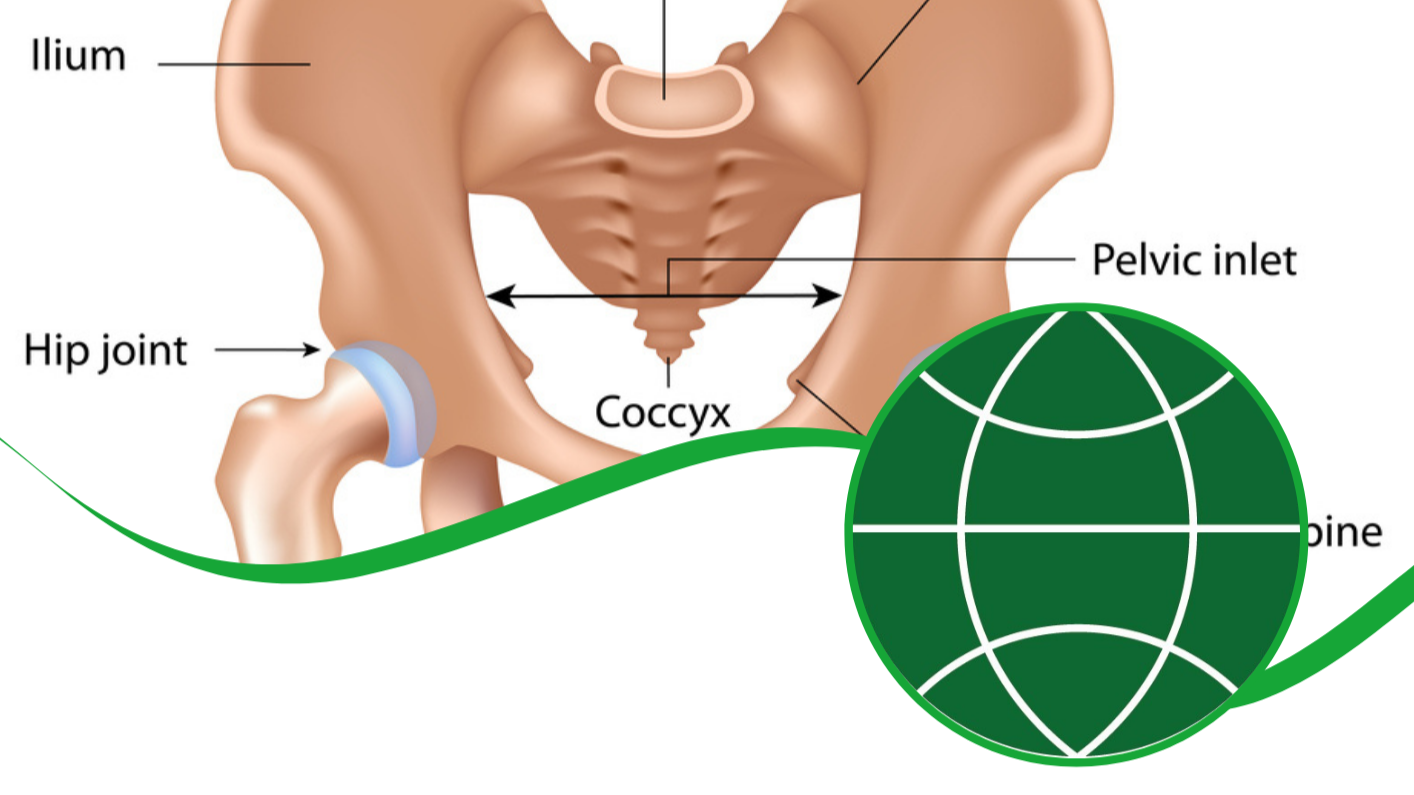
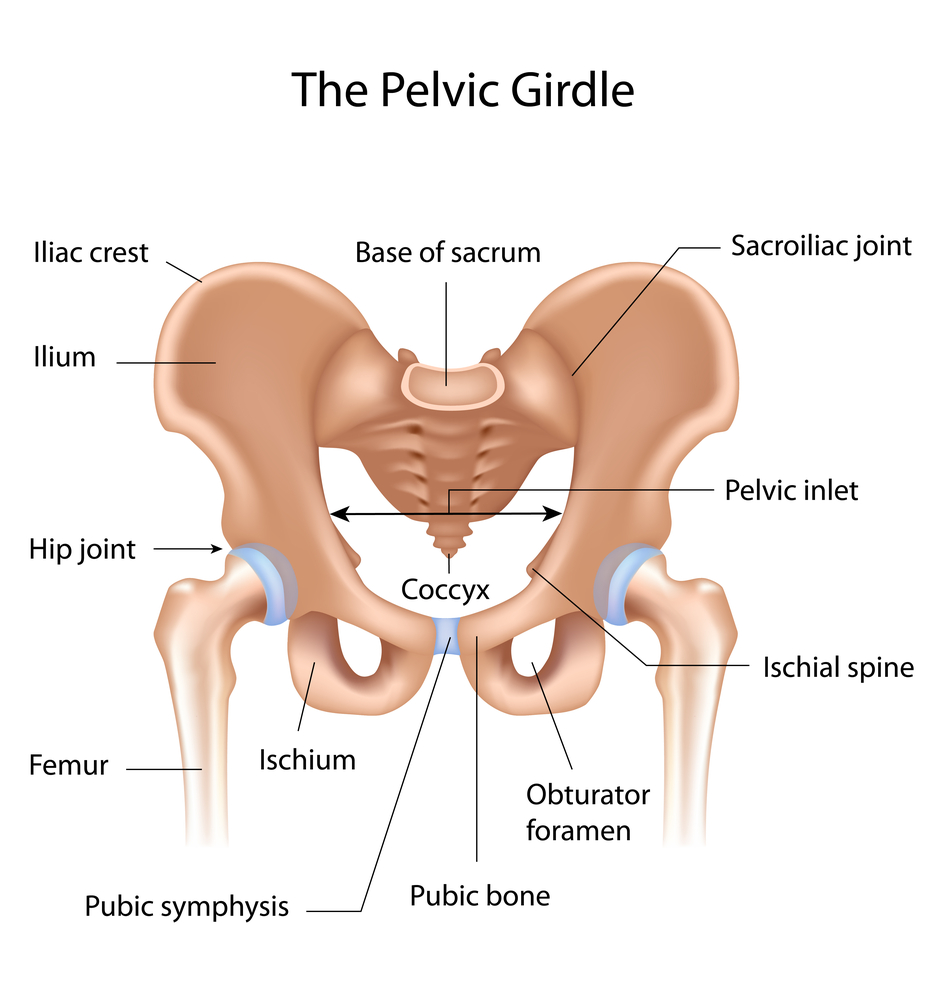
The correct diagnosis and treatment of these conditions may be challenging. This is due to the complexity of the anatomy around the hip, pelvis and abdominal area, as well as other conditions affecting the hip joint with similar symptoms. In addition, conditions which are not musculoskeletal in nature but that have a similar presentation need to be excluded.
A detailed history will be taken from the patient, followed by a physical examination and imaging including X-rays, MRI, CT or ultrasound scanning. The X-rays and CT scans are important to check for degeneration and instability of the pubic symphysis, as well as signs of any structural changes or degeneration of the hip. MRI is used to assess soft tissues, such as cartilage, tendons, ligaments and muscles around the hip and pubic symphysis, as well as checking for any bony oedema or possible stress fractures not normally visible on X-rays. Ultrasound scanning may help in cases where a dynamic exam (where the patient can perform relevant movements during the scan) is necessary for clarification or there is a high suspicion of an abdominal wall hernia.

Non-Surgical Treatment
Treatment is usually non-surgical, focusing on pain relief and involving any combination of the following:
- Rest from all aggravating activities
- Use of non-steroidal anti-inflammatories
- Use of ice
- Physiotherapy involving the use of walking aids if needed, lumbopelvic support belt, exercise therapy to address muscle imbalances, range of movement and core stability
- Corticosteroid injections
Once symptoms improve, any treatment would be followed by a gradual return to activities. Treatment of this condition can be extremely difficult in elite athletes due to the length of time spent away from their sport and the risk of compromising their career.
Surgical Treatment
Where non-surgical methods fail to help resolve symptoms, there are possible surgical procedures, both open and arthroscopic, which may be considered but with variable outcomes. As pubalgia often coexists with FAI, surgery to address both conditions may be performed at the same time.
Examples of surgical procedures used to treat pubalgia include:
- Endoscopic pubic symphysectomy
- Open curettage of the symphysis
- Wedge resection
- Release of adductor longus tendon with or without partial rectus abdominis release
- Placement of extraperitoneal retropubic synthetic mesh
- Inguinal neurectomy
- Arthrodesis
What to expect after surgery
Recovery following arthroscopic surgery is generally quicker than after an open procedure and hence returning to activities is usually also possible earlier. Any return to sport will also depend on operative findings, and advice will be provided by the treating hip preservation surgeon and physiotherapist.
There may be limitations to weightbearing and activities during the first two or three months, which will vary amongst surgeons and will depend on operative findings and techniques performed.
Physiotherapy can begin immediately after surgery, gradually increasing range of movement, stability, strength, mobility and function over a period of up to six months, depending on the surgery performed and individual aims.