Patient Information from ISHA – The Hip Preservation Society
Hip Dysplasia / Developmental Dysplasia of the Hip (DDH)
Hip Dysplasia / Developmental Dysplasia of the Hip (DDH)
Definition
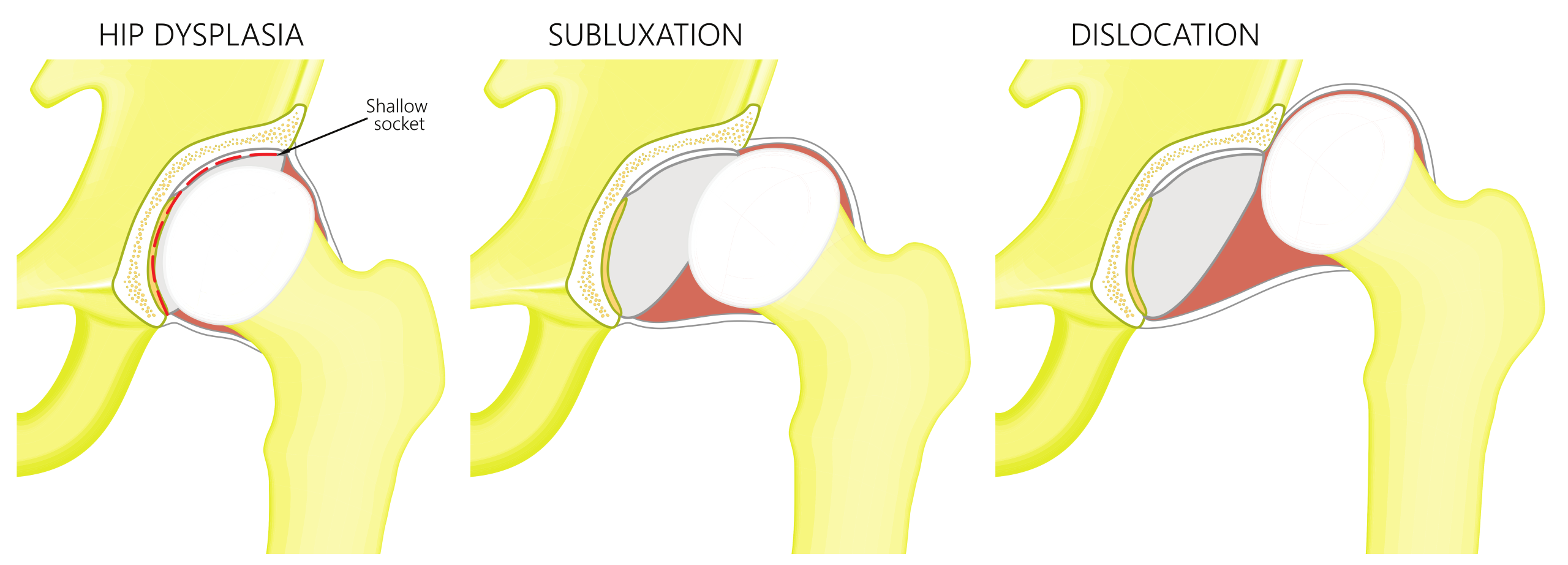
This condition involves the abnormal development (dysplasia) of either one or both hip joints. The shape and/or orientation of the femoral head or socket (acetabulum) may be affected to varying degrees. This abnormality, which is generally present at birth and is more common in females, results in displacement of the hip joint, ranging from partial displacement (subluxation) of the femoral head to a fully dislocated hip. If the hip joint is unstable and dislocated, a diagnosis is more likely in childhood when the condition is better known as “developmental dysplasia of the hip (DDH)”. Conversely, where the socket is stable enough to hold the femoral head in place, an awareness of any such deformity may not be discovered until adolescence, or even adulthood, when symptoms are first reported – the condition may then be known as “acetabular dysplasia”.
Signs and Symptoms
- Hip or leg pain, which may be long standing or aggravated by injury
- Left untreated, there may be the onset of joint degeneration and/or deformity
- Evidence of past growth disturbances
- Avascular necrosis (AVN)
- Residual deformity of the acetabulum/socket
Diagnosis
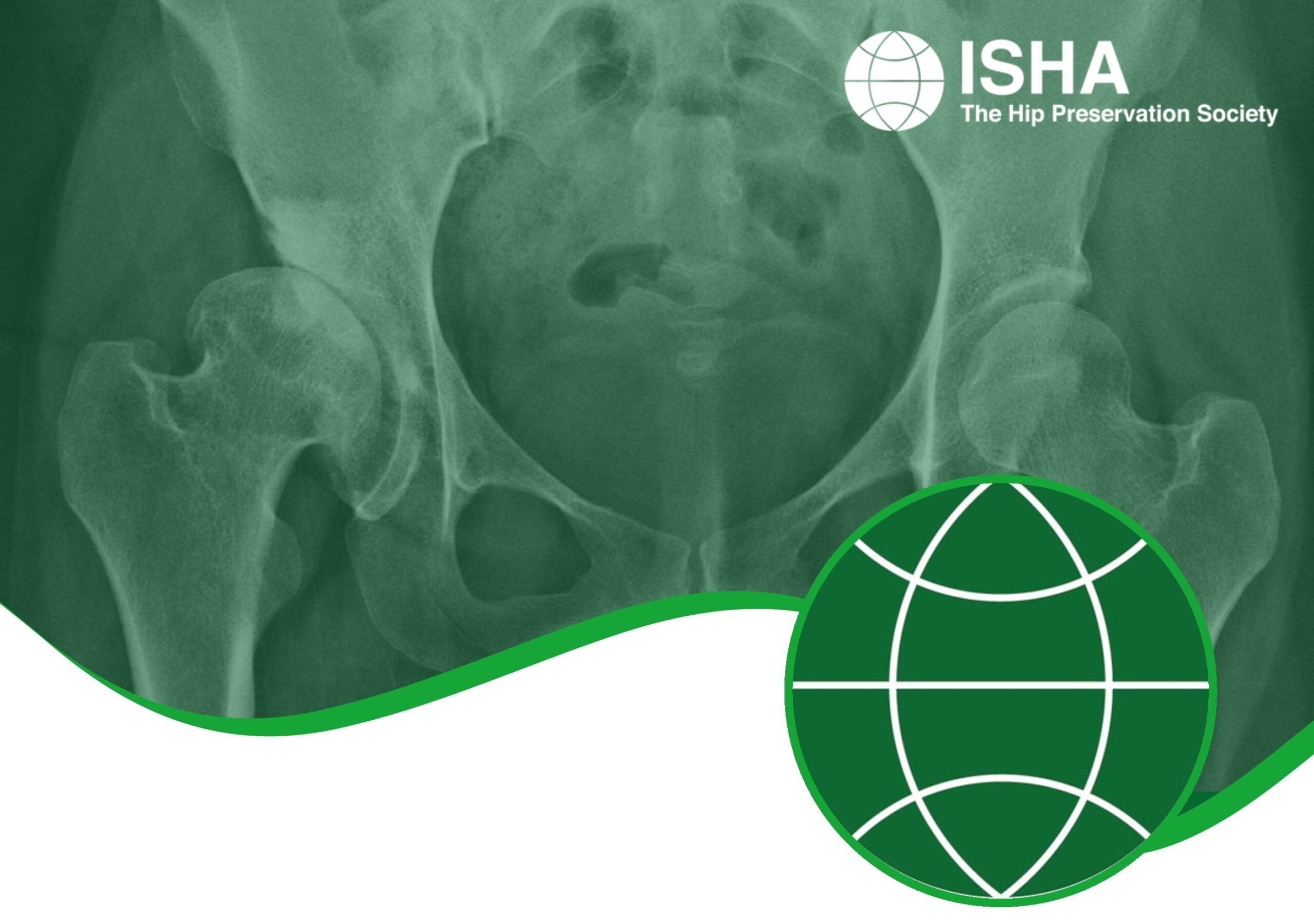
X-rays are frequently used for confirming the presence of hip dysplasia, but MRI and CT scanning may also be recommended. A hip arthroscopy may be performed to further examine the joint, as well as treating certain aspects of the condition.
Pelvis x-ray showing a normal left hip and a completely dislocated right hip (due to DDH)

Non-Surgical Treatment
Physiotherapy may be helpful, including activity modification, pain management, overall postural awareness and improvement, and exercises aimed at improving any muscle imbalances and weakness.
Other conservative treatments may include weight management, nutritionist input, cessation of smoking and general lifestyle advice.
Interventional radiology using image guided local anaesthetic and corticosteroid injections in and around the hip joint may be suggested alongside other non-surgical measures.
Surgical Treatment
Any hip preservation treatment would aim to improve alignment of the hip joint and hence enable the patient to maintain activity levels, mobility and function. In turn, this would delay the onset of problems in later life, including wear and tear of the joint cartilage leading to osteoarthritis and the possible need for joint replacement surgery.
If the acetabulum has not developed correctly and is not deep enough, surgery may be needed to improve alignment of the femoral head – a socket which is too shallow will not provide enough stability for the femoral head. This may be performed in adulthood either due to residual hip dysplasia or following a delayed diagnosis of DDH. This surgery is more challenging and specialist, and is likely to involve some form of pelvic osteotomy – rotating or bending part of the pelvis to better orientate and/or deepen the acetabulum to cover the femoral head. There are a range of different pelvic osteotomies – a periacetabular osteotomy is the most commonly performed in adults. If there is a more subtle deformity of the acetabulum, known as “borderline dysplasia”, a hip arthroscopy may be an alternative.
As a result of hip dysplasia, the femur may develop with abnormal rotational or angular deformities. These may require correction with a femoral osteotomy where a cut (osteotomy) is made through the upper part of the femur. The alignment of the femur is then corrected, and a long rod (nail) is inserted into the bone, holding it in place whilst the osteotomy heals. The rod does not necessarily need to be removed once the bone is fully healed.
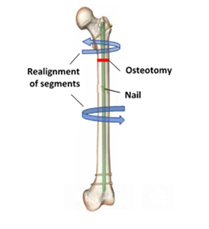
Diagram illustrating femoral osteotomy
If a symptomatic hip joint with malalignment issues is left untreated, any abnormal biomechanics may lead to altered stress distribution within the joint, causing damage to other structures, including the articular cartilage. This may result in early onset osteoarthritis. Depending on the extent of cartilage damage, hip preservation treatments may no longer be appropriate, and a hip replacement may be the only option.
What to expect after surgery
This will vary depending on which surgery was performed, whether any immobilisation is required after surgery, and the preferences and recommendations of the treating hip preservation surgeon. It is also possible that further surgery may be needed, such as removal of metal work. Following any procedure for hip dysplasia there is likely to be a lengthy period of rehabilitation.
There may be limitations to weightbearing and activities during the first two or three months. These will vary amongst surgeons and will depend on what is found during surgery and techniques performed.
Physiotherapy can begin immediately after surgery, gradually increasing range of movement, stability, strength, mobility and function over a period of six to twelve months, depending on the surgery performed and individual aims.