Patient Information from ISHA – The Hip Preservation Society
Ischiofemoral Impingement
Ischiofemoral Impingement
Definition
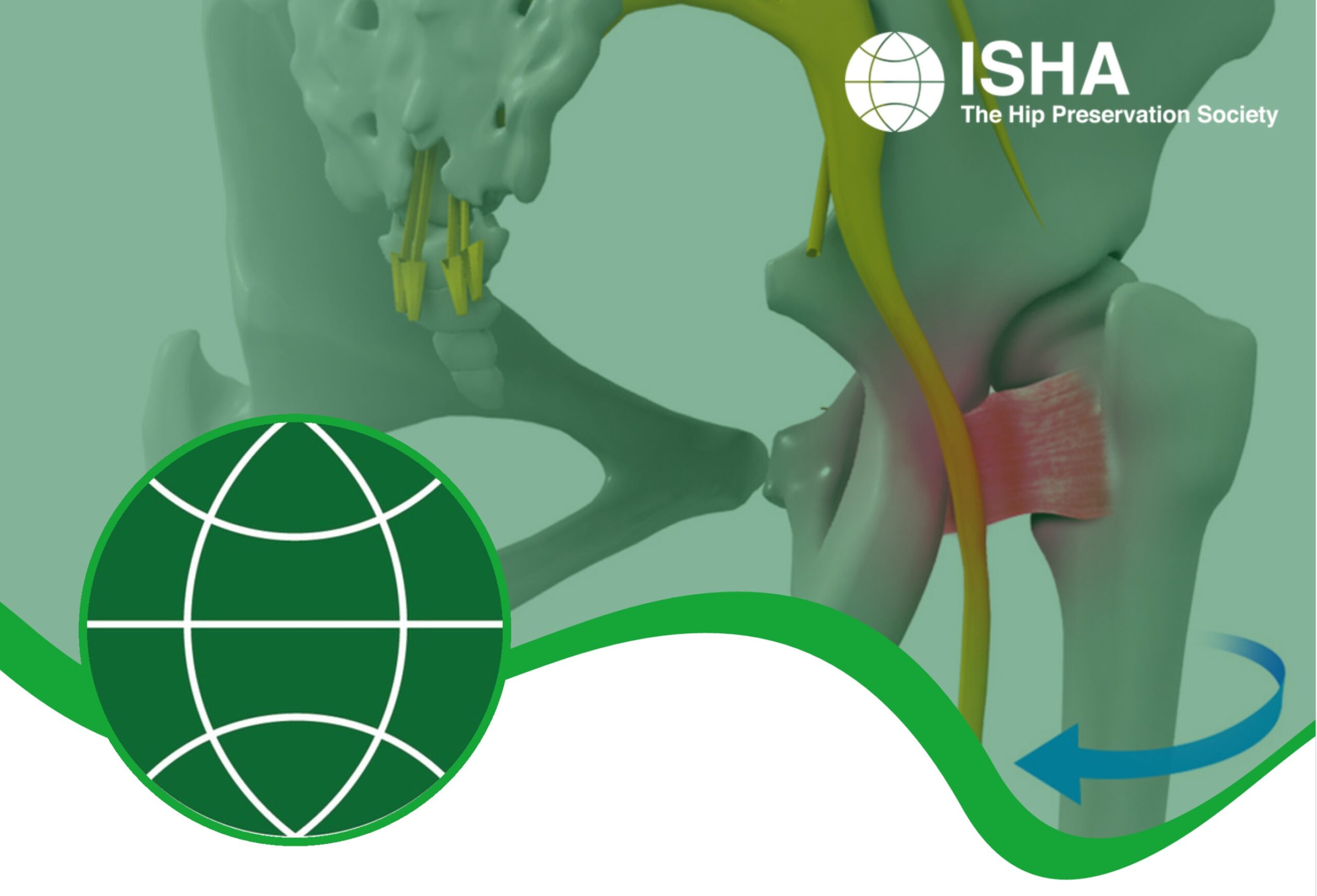
Ischiofemoral impingement, which is rare and more commonly seen in females, results from entrapment of soft tissues caused by narrowing of the space between the pelvis (at the outer edge of the ischium) and the upper end of the femur (at the lesser trochanter). This narrowing may result from:
- a bony abnormality present since birth;
- strenuous repetitive activities;
- arthritic changes; or
- following hip replacement surgery.
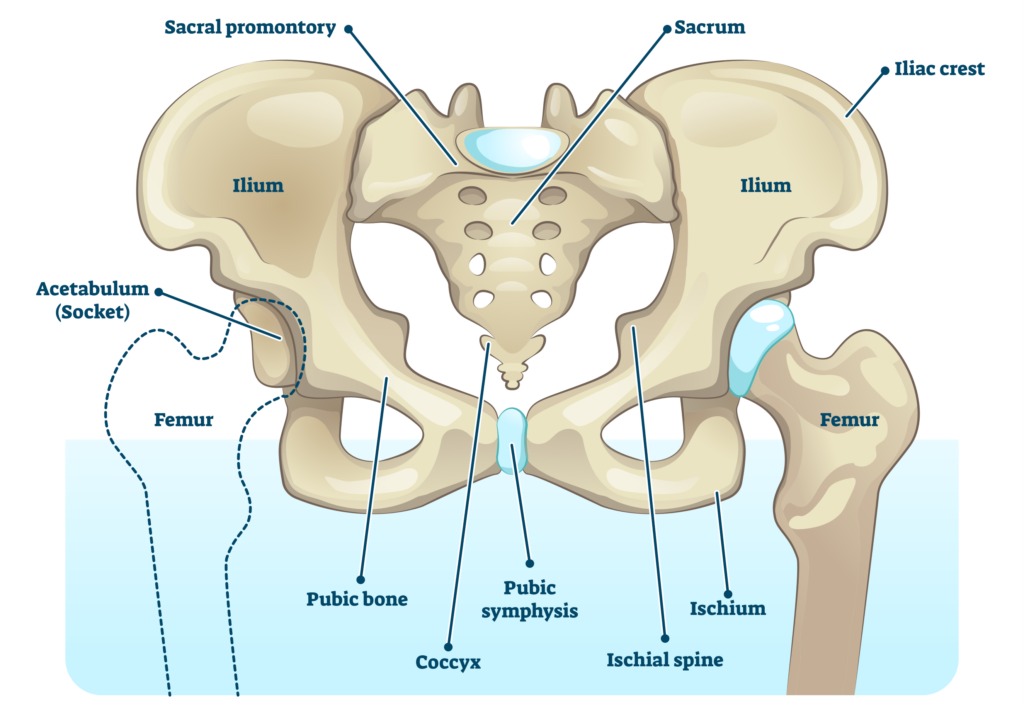
Diagram of the pelvis showing location of the ischium and femur
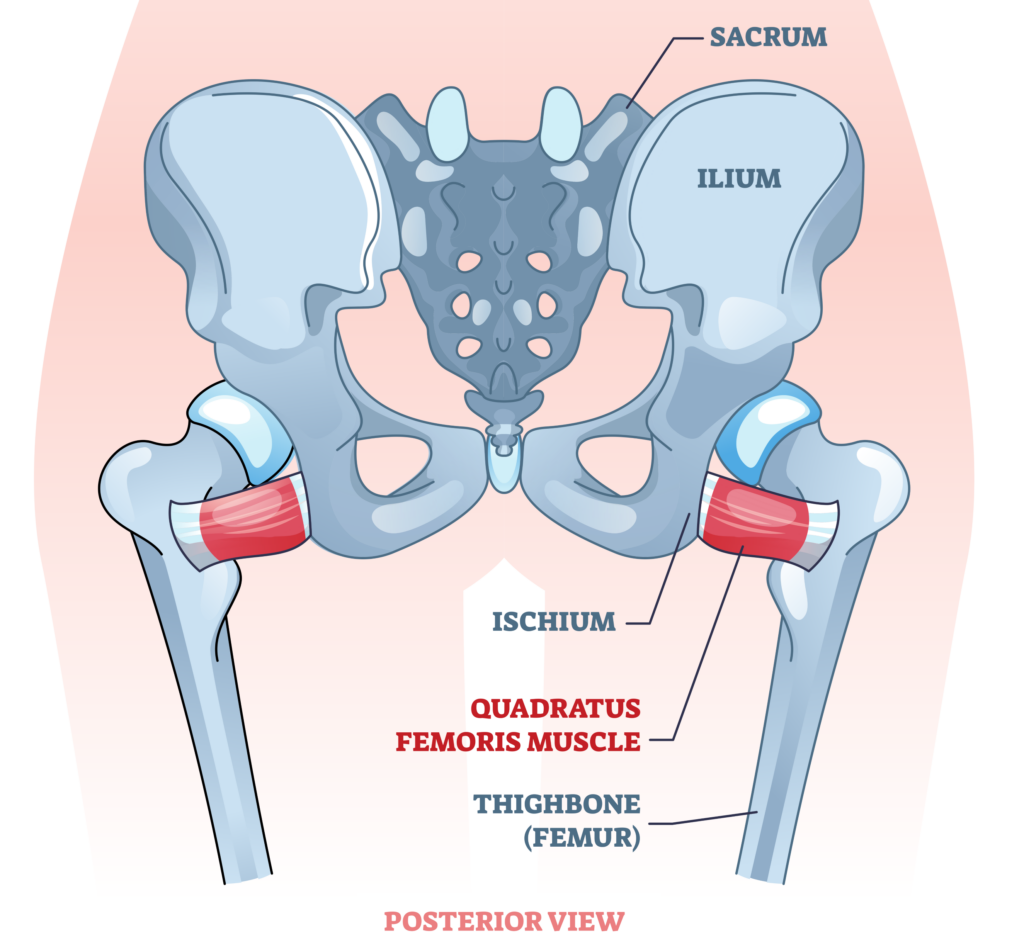
Illustration showing location of the quadratus femoris muscle
Signs and Symptoms
Pain may be in the lower buttock, groin or inner thigh, and is often accompanied by a sensation of clicking, locking or snapping when walking, and often more specifically when the leg is outstretched behind the body. Pain may also mimic sciatica. Often, symptoms will have worsened over a long period of time.
Diagnosis
Ischiofemoral impingement is not easy to diagnose. Specific tests performed during a physical examination may provoke the pain usually experienced. An assessment of movement and walking ability may also provide clues as to the underlying cause of pain. X-rays of the pelvis together with MRIs to assess any effects on soft tissues are likely to be required before a diagnosis is reached. Where an initial diagnosis is not possible in spite of suggestive symptoms, repeat MRIs over time may later confirm changes consistent with the presence of ischiofemoral impingement. Delayed diagnosis may lead to the development of further damage within the hip joint, such as osteoarthritis, as well as the onset of chronic back pain resulting from altered postures and gait in a bid to avoid pain.
Non-Surgical Treatment
- Correction of any differences in leg length
- Physiotherapy addressing any muscle imbalances around the hip and pelvis, with particular attention to strengthening of the hip abductors
- Pain management
- Image guided corticosteroid injection
Where conservative measures fail, hip preservation surgery may be considered.
Surgical Treatment
Surgical management of ischiofemoral impingement will vary according to what soft tissues are affected and damaged, and what correctable bony abnormalities exist. Many of these conditions are described under the relevant sections and hyperlinks are added where appropriate. Treatment could include:
- Gluteal or other tendon repair or transfer
- Femoral osteotomy for the presence of any rotational abnormality of the femur
- Arthroscopic removal/reduction of lesser trochanter of femur
- Open ischioplasty – removal of bone from the ischium to prevent further impingement
- Hamstrings debridement and repair
What to expect after surgery
Recovery following arthroscopic surgery is generally quicker than after an open procedure and hence returning to activities is also easier. Any return to sport will also depend on operative findings, and advice will be provided by the treating hip preservation surgeon and physiotherapist.
There may be limitations to weightbearing and activities during the first two or three months, which will vary amongst surgeons and will depend on operative findings and techniques performed.
Physiotherapy can begin immediately after surgery, gradually increasing range of movement, stability, strength, mobility and function over a period of up to six months, depending on the surgery performed and individual aims.